Somewhere along the way, our achievable goal of "flattening the curve" for COVID-19 has mutated into "finding a cure," which is perhaps an impossible one. Public health and economic policy must be based on reality, not starry-eyed wish-making. Otherwise, people's lives and livelihoods are in grave danger.

The mayor of Los Angeles has said that his city will "never be completely open until we have a cure" for the coronavirus. What planet is he on? (Planet Hollywood?)
For the past couple of months, public health officials and politicians quite rightly told us that some sort of social distancing policies must remain in place in order to "flatten the curve." This was the right thing to do because COVID-19 was threatening to overwhelm our healthcare system. The point of flattening the curve isn't necessarily to decrease the total cumulative number of cases (though, that's a nice side effect if it happens). Instead, the point is to slow down the rate of infection.
But, as Barstool Sports founder Dave Portnoy noted in a profanity-laced tirade posted on Twitter, somewhere along the way, our goal of flattening the curve has mutated into "finding a cure." He's right to be mad. This is utterly misguided for at least three reasons.
First and foremost, there may never be a cure for COVID-19. Though there is a bona fide cure for hepatitis C called Sovaldi, this is an exception to the general rule that viruses are extremely tricky and difficult to treat. That's because most drugs that target viruses also damage our own cells. Despite decades of research, the influenza vaccine is mediocre (e.g., vaccine efficacy for the 2019-20 flu season is so far estimated to be 45%), and the antiviral drug Tamiflu is marginally better than doing nothing. Remdesivir, the leading antiviral drug against the novel coronavirus, is more like Tamiflu than Sovaldi.
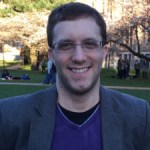
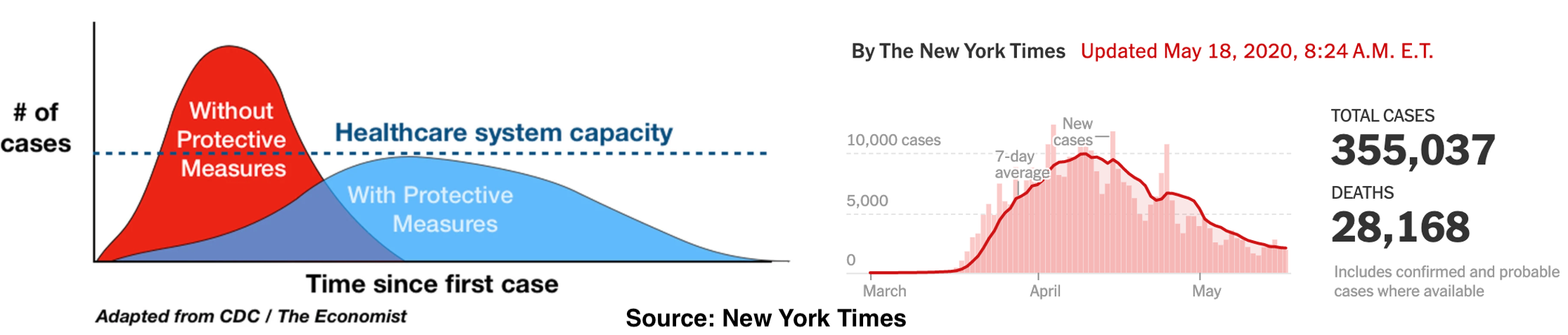
Second, the goal of flattening the curve has largely been achieved. The left-hand figure below visually depicts what is meant by "flattening the curve." Note that the area under the curve (representing the total number of cases) isn't necessarily any smaller; it's just flatter. The right-hand figure depicts actual data on new COVID cases in New York. The curve has been flattened. Once again, the goal is to slow the spread of infection as to avoid overwhelming hospitals, not prevent infections entirely (which is a fool's errand).
Third, there are real social, economic, and public health costs to the lockdown. For some reason, a substantial number of Americans are pretending that COVID-19 is the only thing that kills people. This is false. The pandemic and lockdown have had an enormous impact on mental health, with researchers finding that 28% of people in 2020 screen positive for serious mental illness, compared to just 3.4% in 2018. Recessions and unemployment are also linked to suicide. Public health officials across the U.S. are noticing spikes in opioid overdoses. Poverty and stress, both of which will increase as unemployment rates skyrocket to Great Depression levels, have pernicious effects on public health.
None of this is meant to argue that every city and state should open up everything for business immediately. A cautious approach is warranted, particularly in dense urban areas like New York City. Temporary and well-defined social distancing policies (with explicit end dates) occasionally may need to be reimplemented. Those who are especially vulnerable, such as the elderly and people with underlying health conditions, may want to practice more restrictive social distancing.
However, the rest of society needs to move on. There comes a tipping point in which the socioeconomic and public health costs of the lockdown exceed the benefits. We have now reached that point, which is why we can no longer continue waiting indefinitely for a cure that may never come.