Disparities in healthcare are increasingly a hot topic in the journals. Two recent studies demonstrate disparity but identify very different actionable causes. As with all healthcare, it is more complicated and entangled than a single narrative or lens can explain. The data dots are correct, but there is more than one way to connect and explain them.

Disparities in managing chemotherapy
The study, published in Health Affairs, sought to identify a “practice-level” measure of the racial inequity within two performance metrics promoted by CMS for oncology patients – the incidence of chemotherapy-related emergency department and hospital admissions. The data set included all fee-for-service Medicare beneficiaries treated with chemotherapy between 2016 and 2019 [1]
- 1,166,746 beneficiaries
- 2,436,501 chemotherapy episodes
- 4,862 practices
The mean age was 74, roughly half women and 10.8% were black, and 13.8% received both Medicare and Medicaid (a rough measure of income and disability). The researchers presented data for the entire cohort and a subset whose number of patients treated was greater, and as a result, calculations were more consistent. In the case of both ED and hospital admissions, larger practices yielded more reliable estimates. While the researchers reported all their findings, I will confine this report to the 8.8% of practices, treating 54% of all patients and 74% of all Black patients. Their first “model” was adjusted only for clinical parameters, e.g., age, gender, and comorbidities.
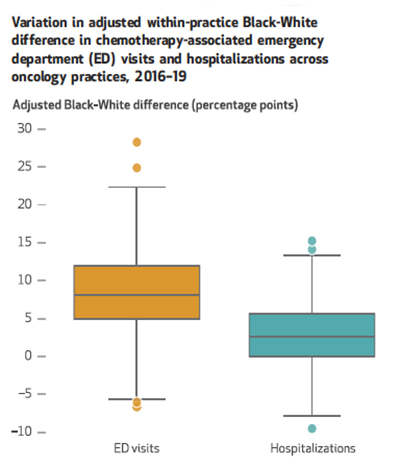 Black patients had 8.1% more Emergency Department admissions for chemotherapy-related problems. [2]
Black patients had 8.1% more Emergency Department admissions for chemotherapy-related problems. [2]- Black patients had 2.7% more hospitalizations for chemotherapy-related problems.
After adjusting for socioeconomic variables, e.g., education, income, residency both disparities were reduced
- Black patients had 3.7% more Emergency Department admissions
- Black and White patients had no difference in hospitalizations
- Dual eligible beneficiaries, irrespective of race, had 13.8 % Emergency Department admissions
Those are the data dots. Here is what the researchers concluded in connecting them.
“On average and in most practices, Black patients had higher rates of chemotherapy-related ED visits and hospitalizations than White patients, suggesting that quality of oncology care may be worse for Black patients.”
They go on to acknowledge the reduction in apparent inequity from adjusting for socioeconomic factors, but as they write and the editors highlighted,
“If inequities are obscured by adjustment for socioeconomic variables, then opportunities to address them will be missed.”
Of course, all of this rests on clinical and socioeconomic adjustments. Did the researchers fully adjust for clinical differences? Or was there a factor not accounted for that might tip the inequity balance? For that, we turn to a study published a few days earlier in the journal Cancer.
Disparities in Baseline Health
As the first group of researchers, the authors of the article in Cancer were also concerned about the disparities in outcomes for Black patients. They noted that even when adjustments are made for the stage of cancer, outcomes for Black patients are worse than all other racial and ethnic groups, except for indigenous Americans. The dataset was the Cancer and Aging Resilience Evaluation (CARE) Registry at the University of Alabama at Birmingham – a cancer registry of adults age 60 or older with a GI malignancy; the data are from 2017 to July 2021.
This data was not, as in the first study, administrative coded information but collected prospectively from the patients. In addition to the usual clinical and socioeconomic demographics, the study collected self-reported data on patient frailty – the ability to navigate the activities of daily life. [3] There were 553 patients, 23.1% Black, the rest non-Hispanic White. Median age 70. All had a GI cancer. Black patients were slightly younger at 68.7, with lower levels of educational attainment and higher levels of disabled employment status. There was no statistically significant difference in the stage of their disease from the non-Hispanic Whites.
There was one glaring difference; Black participants had “a higher prevalence of frailty (50.0% vs. 32.9%.” When adjusted Black patients were 2.59 times more likely to be frail than White participants. Black patients were less able to walk one block, to carry out the “instrumental” activities of daily life, e.g., managing their finances, housekeeping, laundry, preparing meals, and more likely to be dependent upon others in those activities.
Here is an intriguing fact: White patients were more likely to be hearing impaired, and Black patients were more likely to be visually impaired. Perhaps this is too broad a brush, but hearing loss results in isolation, visual loss in dependence. The researchers concluded,
“The increased prevalence of frailty in older Black participants may at least partially mediate known differences in cancer outcomes and warrant further investigation.”
With both studies now in hand, let us return to the conclusion of the first group of researchers. Their data did suggest that the “quality of oncology care may be worse for Black patients,” but the second study suggests that they didn’t have all the data. A two-fold difference in frailty would seem to easily overwhelm the 8% disparity in chemotherapy-related admissions. Could adjusting for frailty significantly reduce that 8% difference found in the first study so that the problem was not the quality of care but the patient's resilience?
The first study does hint at this possibility. Remember that those patients on Medicare and Medicaid had the highest incidence of chemotherapy-related admissions, 13 plus percent. Medicaid provides care for the poor and the chronically disabled, the frailer members of our society.
Those frailties may be due to a lifetime of stress and other components of “structural racism” that have worn these individuals down, but frailty cannot be treated with a pill or an operation. Frailty shifts the metric away from physicians who can do little other than make social service referrals and focuses on services supporting patients' other needs to tilt the playing field in support of all patients.
[1] The focus was solely on black and white patients because the other group numbers were too small. Hormonal therapy was not considered chemotherapy.
[2] No mention of the nature of these problems is made. Intractable nausea and vomiting, fever, and abnormal blood counts are problems bringing chemotherapy patients into the ED or hospital.
[3] This includes falls, functional status limitations, physical and mental function, nutrition, social support, cognitive complaints, social activities, polypharmacy, and comorbid conditions.
Source: Measuring Racial Inequities In The Quality Of Care Across Oncology Practices In The US Health Affairs DOI: 10.1377/hlthaff.2021.01594
Racial disparities in frailty and geriatric assessment impairments in older adults with cancer in the Deep South: Results from the CARE Registry Cancer DOI: 10.1002/cncr.34178
