In spite of study after study and the writings of expert after expert over the last 25 years, we, as a society, have failed to provide for our own security in the face of a potential public health threat. We have failed to supply and maintain our strategic national stockpile, we have consistently underfunded our public health infrastructure and we have underfunded our hospitals' preparedness.

Let’s first discuss the Strategic National Stockpile (SNS). The Department of Defense maintains its own stockpile and has done so since the 1930s. The thinking that led to DoD’s preparedness ultimately led to the formation of today’s SNS for the US population at large. In 1998 Bill Clinton signed a law forming the National Pharmaceutical Stockpile. In 2003, after 9/11 and the anthrax attacks, the role for the stockpile expanded considerably and became the Strategic National Stockpile managed primarily by CDC under the Secretary of Health and Human Services and the Department of Homeland Security. The stockpile is kept at various regional locations around the country. It stocks a wide variety of pharmaceuticals and vaccines as medical countermeasures against biological attack. A summary of these holdings can be found here. Many of those countermeasures were purchased by the stockpile under BARDA. The NIAID and BARDA were responsible for a large fund called Project Bioshield established in 2003, under President George W. Bush, to support research into these medical countermeasures. NIAID, with over $5 billion in funding for Project Bioshield, established a number of regional centers of excellence to study dangerous pathogens that could potentially be weaponized. This funding established sites that were equipped to handle these pathogens under strict security – physical and biological. The research yielded important basic scientific understandings of these dangerous pathogens and toxins, but little in the way of actual vaccines and countermeasures. The latter came mainly from small biotechs who believed that the SNS might serve as a business model for their R&D. (In my view, they were, in the main, disappointed).
 The Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) is the organization that decides what goes into the stockpile. They have expanded the stockpile over the years to cover needs for other situations such as hurricanes and earthquakes for example. They have also stocked key hospital supplies like masks, gowns and ventilators in preparation for a pandemic like Ebola, Zika or influenza. In their budget, maintenance of inventory is an essential item.
The Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) is the organization that decides what goes into the stockpile. They have expanded the stockpile over the years to cover needs for other situations such as hurricanes and earthquakes for example. They have also stocked key hospital supplies like masks, gowns and ventilators in preparation for a pandemic like Ebola, Zika or influenza. In their budget, maintenance of inventory is an essential item.
Funding for this overall effort began with an infusion for a 10 year period in 2003 ending in 2013. After that, congress moved Project Bioshield to BARDA and funded it on a reduced year over year basis. In spite of the reduced funding, BARDA has been a stalwart in our effort to find and stockpile medical countermeasures. Early on, BARDA was constrained to funding antibiotic R&D only for those products that clearly had an application as medical countermeasures. That expanded later to include antibiotics active against resistant infections. This was clearly appropriate given the public health threat of these infections. Initially, BARDA was also constrained to focus only on those products that were entering late stage clinical development. Now, BARDA has become a key funder of CARBX – focused on early stage research of antibiotics. They have also been able to support “portfolios” of antibiotic research within companies encompassing late stage as well as early stage R&D. In a recent move, perhaps to address the suffering antibiotic marketplace, BARDA has entered an agreement to fund Paratek’s omadacycline as an agent for the treatment of drug resistant anthrax with a commitment to ultimately purchase the drug for the national stockpile. It is clear that without BARDA, our antibiotic pipeline would be in even more disastrous shape than it is currently. It is also clear that with additional funding, BARDA could do so much more.
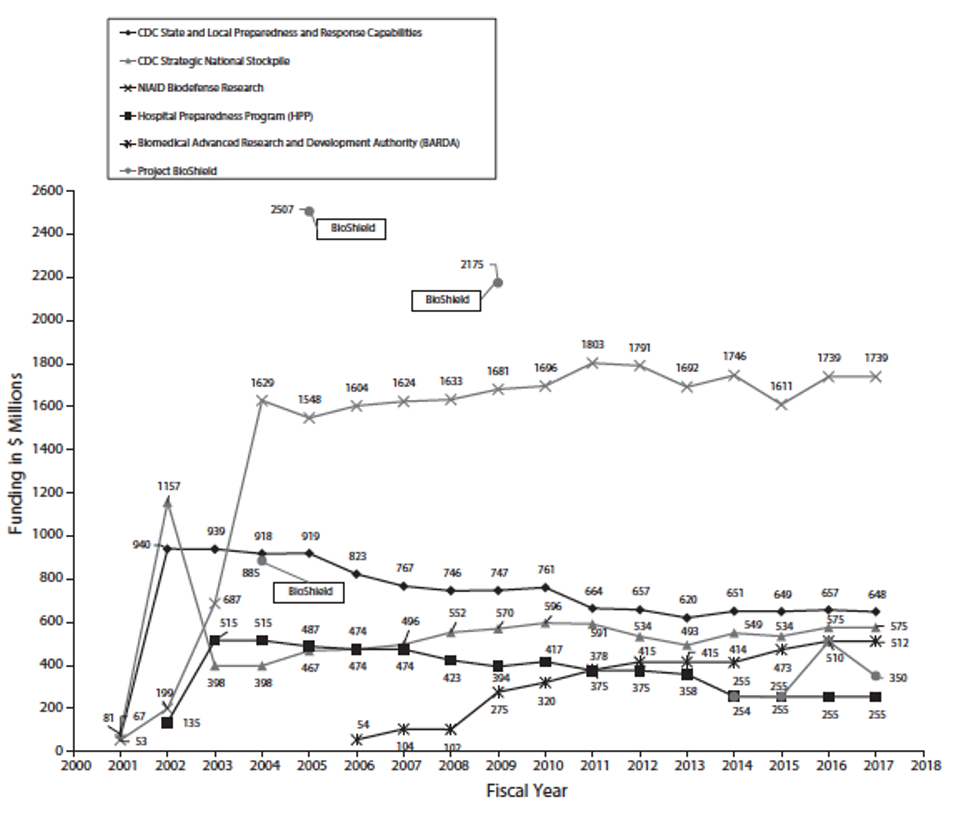
In addition to the SNS, there are funds distributed by the CDC to local public health authorities and to hospitals for preparedness. A history of funding for these various programs is shown in the figure below. If you focus on funding for hospitals, you will see a drastic decrease over time. Funding for these programs has decreased by 30-50% not counting inflation. The years cover both democratic and republican administrations and congressional majorities. Apparently, in spite of strident warnings by both experts and two of their own – Tom Daschle and Judd Greg – government was not willing to invest sufficiently for our future security. (Although the Trump administration proposed cuts to both the hospital preparedness program and to the emerging zoonotic diseases program, congress maintained or even slightly increased funding for these areas in 2018 according to Politifact. Obviously, this was still not sufficient.)
As we slowly emerge from this horrible pandemic, will we learn from our missteps?