
Recently, the New York Times published “How Wildfire Smoke Threatens Health,” for which the theme was ‘’understanding how the airborne remnants of blazes affect human health.” A stimulus may have been a press release from Stanford detailing health effects of the extensive 2020 fires in Northern California. As usual with the popular press, the Times article has some kernels of truth gleaned from a few specialists, but there are also inconsistencies. The most concerning aspect was that the Times article did not draw on published research of the experts they cited. Understanding health effects requires identifying victims, estimating exposures, and considering the physiological mechanisms involved.
Cleland and others wrote that estimating health impacts requires two types of information: rates of exposure and response concerning the most harmful elements. The former involves knowledge of human behavior during a wildfire event, including avoidance strategies and indoor conditions. The “harmful elements” in ambient smoke have not been identified. She noted that her conclusions were “sensitive to assumptions.”
Montrose conducted experiments on asthmatic children exposed to indoor wood-burning, with or without indoor air filtration. They concluded that “improved indoor air quality did not affect quality of life measures.” This finding must be tempered with the study's small size and the more efficient combustion of indoor appliances relative to wildfires.
Gould wrote about experiments with using cleaner space-heating fuels in New York City apartment buildings. They concluded that although outdoor air quality (PM2.5) was improved, indoor air quality was unchanged in either upper or lower-floor apartments. However, the pollution levels were well below health standards.
Gould was also the lead author of a 2024 comprehensive review of the health effects of wildfire “fine particles,” denoted PM2.5. The review provides useful risk estimates for mortality and hospitalization that showed widely disparate findings. In the table, I show their weighted-average risk estimates based on same-day incremental exposures of 10 µg/m3 (approximately twice ambient levels), considering subsequent days might have increased those estimates.
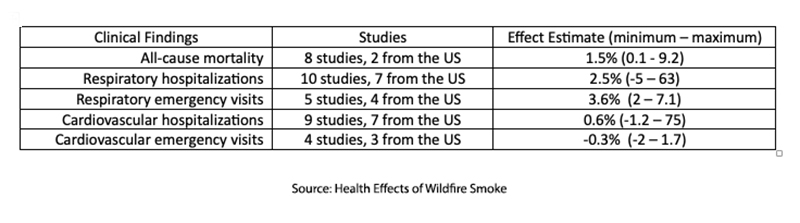
In other words, doubling PM2.5 exposure on a single day may cost a few percentage points in respiratory health. These weighted averages are statistically significant except for cardiovascular emergency visits, but relying on any of them would be fraught. The review presented dose-response relationships between PM2.5 and emergency department visits; there was no relationship for all-cause visits but a strong linear relationship with asthma visits.
The review lists some of the most toxic components of wood smoke not identified by PM2.5, e.g., black carbon or organic species like benzo(alpha)pyrene (an important carcinogen). PM2.5 is used for regulatory purposes without regard to emission sources or particle composition. The Air Quality Index (AQI) cited by the Times is a mishmash of all EPA-regulated pollutants and again fails to consider pertinent components of polluted air – it has a place in your daily weather reports, not in scientific publications.
PM2.5 is a Poor Measure
What does PM2.5 measure? Answer: Whatever is collected by an EPA-approved device designed to exclude particles whose aerodynamic diameters exceed 2.5 µm. PM2.5 composition varies geographically, but typically is about 30% dust, 30% organics including black carbon, 30% inorganics ions such as SO4, NH4, NO3, and a smattering of metals. Concerning climate change, black carbon absorbs heat, but SO4 reflects sunlight. Thus, wildfire effects on global warming cannot be indicated by PM2.5. (Combustion of any carbon-based material emits CO2.) Whether climate change per se can initiate wildfires is another matter.
The elephant in the room for smoke-health studies is the question of particle size, which is not well-addressed by PM2.5. Gould, among many others, points out the hazards of much smaller particles that can enter the bloodstream and “cause damage at the cellular level.” Lippmann gathered data on the rates of respiratory tract deposition of inhaled particles according to size (in µm).
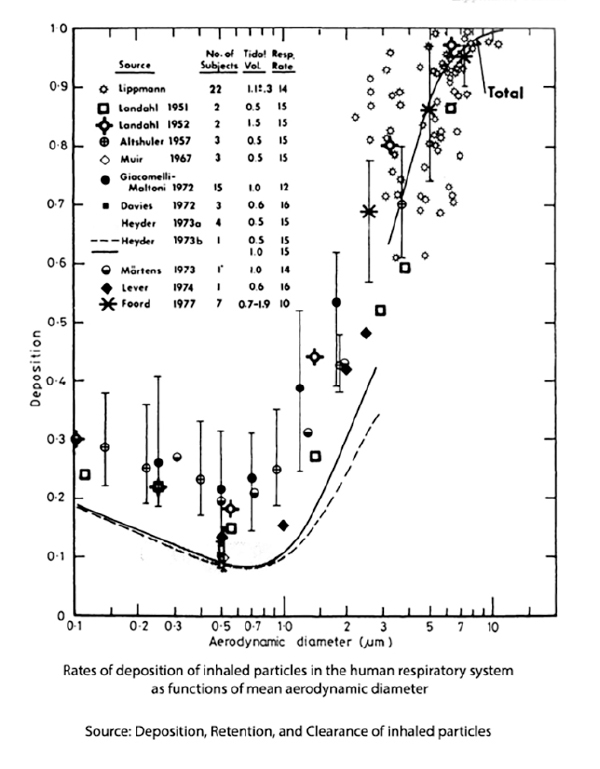
- Deposition of 10 µm particles, PM10, is nearly complete and may be cleared from the upper respiratory tract by coughing, etc.
- About 40% of inhaled PM2.5 is deposited, but only 10-20 % of 0.5 µm particles
- The remainder are not deposited. As a comparison, cigarette smoke particles are generally in the 0.1 – 1.0 µm size range.
While acute health impacts may be associated with regulated PM10 and PM2.5, chronic conditions like cardiovascular disease or cancer are not.
There have been a few attempts to measure the size distributions of wildfire smoke particles, with mixed results. Fine particles average about 0.11 µm; some have found an additional coarse mode at about 12 µm. It is thus apparent that PM2.5 data are not applicable. The characteristics of wildfire smoke depend on the wood species, combustion temperature, and weather. Until more specific ambient measures are deployed, there is little hope that smoke health effects can be understood.
My bottom lines for wildfire health effects are:
- The risk of a highway accident while trying to escape a blaze likely exceeds any daily inhalation risks, absent pre-existing conditions like asthma.
- Respiratory effects may be more important than cardiovascular. Individuals with asthma appear to be especially vulnerable.
- In contrast to cigarette smoking, acute responses to wildfire smoke have been documented, but evidence for chronic or cumulative effects has not.
- No casualties from wildfire smoke inhalation have been identified.
- Data on chemistry and particle sizes during severe smoke episodes are needed but have been woefully lacking.
[1] While there were no mortalities, the study did demonstrate a worsening of pulmonary function, as measured by FEV1 over time. FEV1 is a standard measure of the ability to exhale.


